大家都在搜

手机验证

询价列表
暂时没有已询价产品
大脑中动脉栓塞(脑缺血/MCA
O)+再灌注
企业认证
脑缺血再灌注动物模型
实验目的 和意义:
建立稳定可靠的局灶性大鼠脑缺血再灌注模(MCAO),用于对缺血性神经损伤的治疗和保护机制的研究。
实验原理:利用外科手术方法使大鼠中动脉闭塞,造成局部脑缺血,一定时间后恢复供血形成脑缺血再灌注动物模型。
实验仪器:手术器械,显微镜,专业栓塞线等。
实验内容:
(1)实验动物
SD大鼠,体重250g-300g
(2)实验方法
1.线栓法:
大鼠麻醉,常规消毒,颈部正中切开,分离暴露右侧颈总动脉、右颈内动脉和右颈外动脉,用动脉夹阻断颈内动脉和颈总动脉血流,在颈外动脉远端距分叉约6mm处剪开颈外动脉(远端结扎),向分叉方向插入头端5 mm覆以硅胶的栓塞线,返折颈外动脉使颈外动脉与颈内动脉成一直线,线栓进入颈内动脉,继续向颅内插入约18mm,当感觉到较明显阻力时,说明线栓已到达大脑中动脉起始部,若出现该侧动眼神经麻痹和对侧肢体瘫痪即表示缺血成功。缺血1.5小时后拔出线栓至颈总动脉分叉处,造成缺血再灌注模型。
2.其它方法:开颅法;光化学诱导法等。
(3)评价指标:
1.神经行为学评估;
2.TTC染色,统计梗死灶面积比例;
3.脑组织钙离子浓度检测,
4.其他检测指标。
(4)治疗手段:
由委托方提供治疗方法和治疗药物。
服务周期:根据具体实验方案而定。
结果提交:提交实验报告书、原始数据、图片等。
ABSTRACT
Stroke is the third cause of mortality and the leading cause of disability in the World. Ischemic stroke accounts for approximately 80% of all strokes. However, the thrombolytic tissue plasminogen activator (tPA) is the only treatment of acute ischemic stroke that exists. This led researchers to develop several ischemic stroke models in a variety of species. Two major types of rodent models have been developed: models of global cerebral ischemia or focal cerebral ischemia. To mimic ischemic stroke in patients, in whom approximately 80% thrombotic or embolic strokes occur in the territory of the middle cerebral artery (MCA), the intraluminal middle cerebral artery occlusion (MCAO) model is quite relevant for stroke studies. This model was first developed in rats by Koizumi et al. in 1986 1. Because of the ease of genetic manipulation in mice, these models have also been developed in this species 2-3.
Herein, we present the transient MCA occlusion procedure in C57/Bl6 mice. Previous studies have reported that physical properties of the occluder such as tip diameter, length, shape, and flexibility are critical for the reproducibility of the infarct volume 4. Herein, a commercial silicon coated monofilaments (Doccol Corporation) have been used. Another great advantage is that this monofilament reduces the risk to induce subarachnoid hemorrhages. Using the Zeiss stereo-microscope Stemi 2000, the silicon coated monofilament was introduced into the internal carotid artery (ICA) via a cut in the external carotid artery (ECA) until the monofilament occludes the base of the MCA. Blood flow was restored 1 hour later by removal of the monofilament to mimic the restoration of blood flow after lysis of a thromboembolic clot in humans. The extent of cerebral infarct may be evaluated first by a neurologic score and by the measurement of the infarct volume. Ischemic mice were thus analyzed for their neurologic score at different post-reperfusion times. To evaluate the infarct volume, staining with 2,3,5-triphenyltetrazolium chloride (TTC) was usually performed. Herein, we used cresyl violet staining since it offers the opportunity to test many critical markers by immunohistochemistry. In this video, we report the MCAO procedure; neurological scores and the evaluation of the infarct volume by cresyl violet staining.
Transient Middle Cerebral Artery Occlusion (MCAO)
1. Surgery Procedure (Figure 1)
Transient middle cerebral artery occlusion (tMCAO) is performed on 2- to 3-month old male C57Bl/6 mice (22-28g). This protocol was approved by the IRCM bioethics committee animal care. Surgical tools were sterilized by autoclaving (121 °C at 15 psi for 60 min). Between each animal, they were sterilized using the hot bead sterilizer (15 sec). Surgery table and other equipment are sanitized using 70% ethanol.
Two hours before surgery, mice were analgesized with buprenorphine (0.03 mg/kg b.w. i.p.).
Figure 1A.
Figure 1B.
2. Restoration of Middle Cerebral Artery Blood Flow
Before reanesthesia, the neuroscore can be checked to evaluate the success of the surgery.
3. Sham Operation
For sham operations, all procedures are identical except that the occluder is not inserted.
4. Neuroscore
Neurological deficits allow the evaluation of the success of tMCAO just after reperfusion and later the estimation of the degree of severity of the injury. Neurological deficits are scored as previously described 5 and performed at 1, 24, 48 and 72 hr post-reperfusion. An expanded six-point scale is used:
5. Cresyl Violet Staining (Figure 2)
Following PBS solution perfusion, brains are quickly frozen in isopentane and stored at -80 °C. Mouse brains may be also perfused with 4% paraformaldehyde (PFA) depending on the planned immunohistochemistry studies. Cryostat-cuts of coronal brain sections (17 μm) are performed. One section out of every 30 is collected on the same slide to have a representative cerebral injury. For volume quantification, 2 slides are stained by cresyl violet staining and an image analysis system (Scion Corporation, Frederick, MD) was used to evaluate the lesion. The injury volume was calculated in arbitrary units (pixels), and expressed as a percentage of the contralateral non-lesioned area for each section. Other slides are kept at -80 °C for immunohistochemistry studies. Alternatively, PFA-fixed brain can be cut at 30-50 μm using vibratome and the infarct volume measured as recommended by Han et al.(2009)6.
The neuroscore evaluation confirms the success of tMCAO post-stroke and determines the efficiency of the tMCAO post-reperfusion. In our hands, all mice subjected to the intraluminal procedure presented at least a mild consistent curling (neuroscore 2) and the neurological deficits are generally stable up to 72 hr. Most mice exhibit a mild consistent curling (neuroscore 2). Mice showing absence of curling are excluded from the study. However, the neuroscore evaluation does not allow us to distinguish between mice with an injured hippocampus and those with an intact hippocampus.
No mortality was observed during the surgery day, suggesting that subarachnoid hemorrhages did not occur. When subarachnoid hemorrhage is identified in a mouse, this one is systematically excluded from analysis. The use of silicon-coated monofilament from Doccol Corporation, which is smoother than home-prepared monofilaments, increases the success of tMCAO and reduces subarachnoid hemorrhages. Mortality between 24 hr and 72 hr is 14% in this model, as generally reported for 60 min of occlusion. The mortality observed is probably due to a large infarct volume in this mouse strain. A strong lesion reproducibility has also been observed (standard deviation is 15%), which is very interesting to study neuroprotection molecules where their effect(s) could be hidden by the variability of the model.
To evaluate the extent of brain injury following tMCAO, we opted to use cresyl violet staining (Figure 2) rather than TTC in order to have a lot of materials to test relevant markers6. The extent of the lesion is relatively consistent. However, we noticed that in some mice, the hippocampus was injured (around 30% of mice). It is interesting to note that cresyl violet staining can be applied up to 1 week later. In the literature, the percentage of brain infarct varies from one study to the other. It depends on the choice of mouse strain, the anesthesia, the thickness of brain sections, the monofilament used, or the staining used 6, 7.
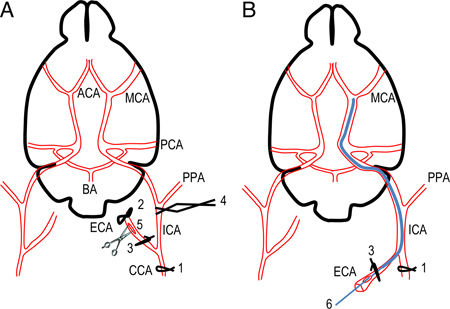
Figure 1. Scheme of the occlusion of the middle cerebral artery using silicon-coated intraluminal monofilament. A. Simplified scheme of mouse brain and cerebral arteries showing successive sutures and clip to prepare the introduction of silicon-coated monofilament. B. The position of monofilament through the circle of Willis is represented. The monofilament is introduced into ICA via ECA to occlude the base of the MCA. ACA, anterior cerebral artery; BA, basilar artery; CCA, common carotid artery; C. Willis, Circle of Willis; ECA, external carotid artery; ICA, internal carotid artery; MCA, middle cerebral artery; PCA, posterior communicating artery; PPA, pterygopalatine artery.
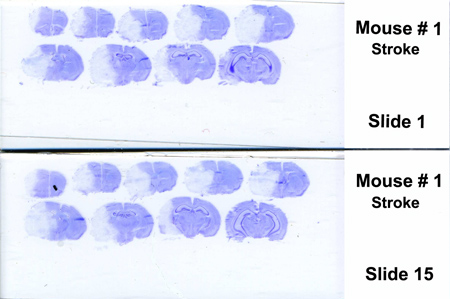
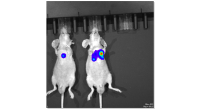
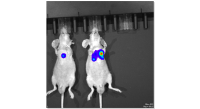
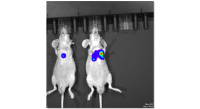
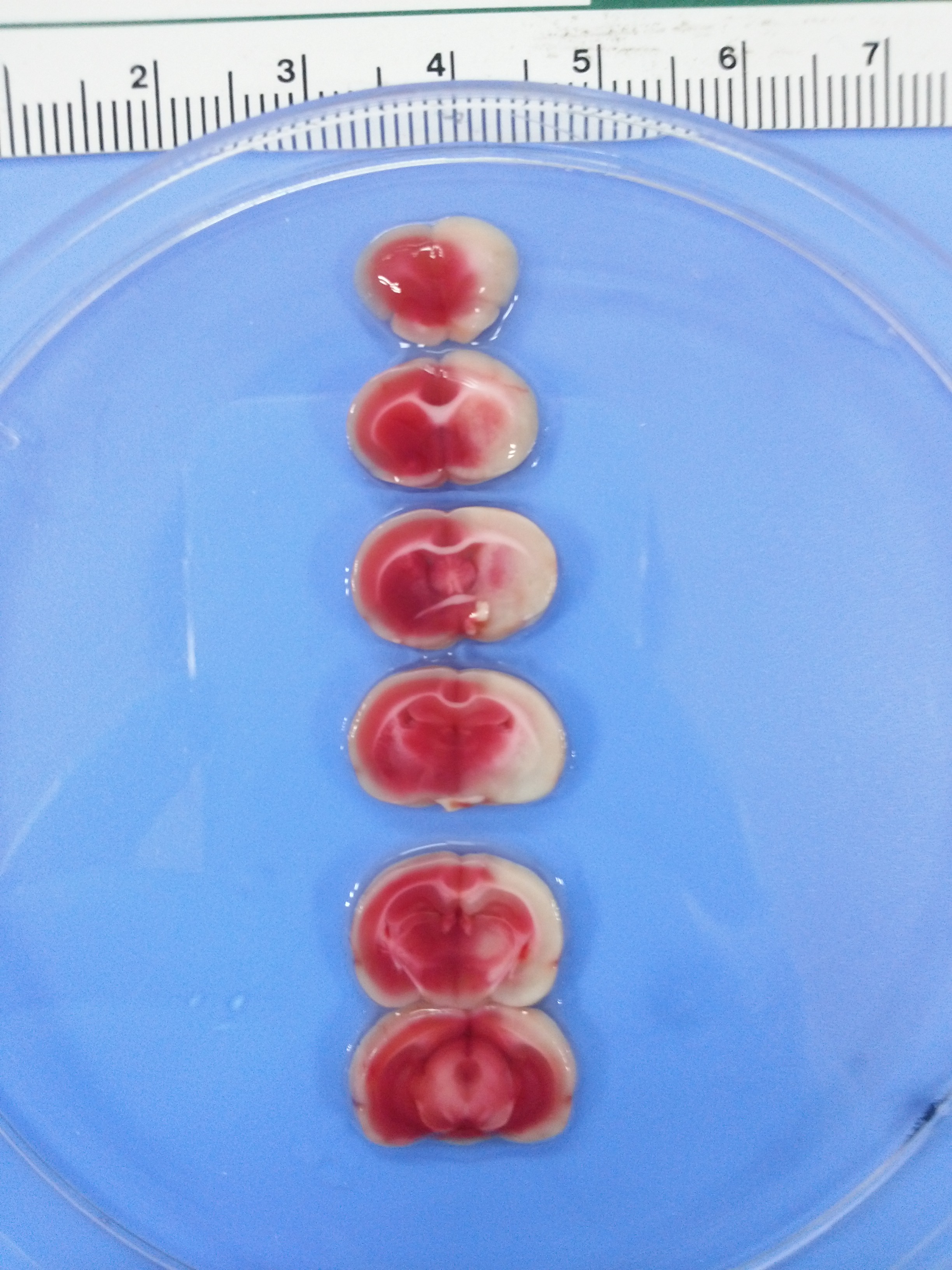
Figure 2. Representative coronal sections of mouse brain stained with cresyl violet after 72 hr post-reperfusion. Infarct area (mainly striatum, cortex and adjacent brain areas) appears in white (unstained by cresyl violet). The injury volume (white part, right hemisphere) was delimited and expressed as a percentage of the contralateral non-lesioned area (left hemisphere).
Different stroke models have been developed to mimic stroke consequences in patients. The choice of the stroke model depends on the biological question. The intraluminal MCAO model mimics one of the most common types of ischemic stroke in patients and is less invasive and more consistent than the Tamura model 4,7. It is a really interesting model for neuroprotection, neurorepair and cell death analyses. The success of the intraluminal model depends on many factors such as animal sex, age and weight, temperature, anesthesia and the time of surgery, which have to be controlled. The physical proprieties of the occluder (tip diameter, length, shape and fexibility) are critical for the consistency of the MCAO 4. Herein, we use the 12 mm-long 6-0 monofilament coated with silicon on 9-10 mm from Doccol Corporation. The great advantage of this monofilament is to reduce subarachnoid hemorrhages and because its length covered all the ICA length, residual blood flow, which comes from the anterior and posterior communicating arteries of the Circle of Willis and PPA, is prevented and the variability in the infarct volume decreases (15% of variability in our hands) 8. The suture of CCA also decreases the variability of the infarct volume 9.
The extent of brain injury following tMCAO can be assessed by different ways. Neurological deficits can be measured as previously mentioned. However, it is difficult to have an efficient measure by this way. The extent of the infarct is commonly performed by TTC staining. More recently, magnetic resonance techniques are also used, a particularly interesting technology for neuroprotective treatments. To understand the underlying cellular mechanisms involved in stroke such as neurorepair, cell death or cell proliferation, the study of different markers by immunohistochemistry is critical and very informative. Thus, our protocol of brain section preparations has the great advantage of allowing these analyses, and minimizes the number of mice used. Moreover, Tureyen et al. 10 have reported that there is good correlation between cresyl violet staining and TTC.
风险提示:丁香通仅作为第三方平台,为商家信息发布提供平台空间。用户咨询产品时请注意保护个人信息及财产安全,合理判断,谨慎选购商品,商家和用户对交易行为负责。对于医疗器械类产品,请先查证核实企业经营资质和医疗器械产品注册证情况。
 询价记录
询价记录